

CardioNerds Journal Club is a monthly forum for CardioNerds to discuss and breakdown recent publications on twitter and are produced with a corresponding infographic and detailed blog post. For more information, check out the CardioNerds Journal Club Page. This Journal Club focuses on the STELLAR Trial

Table of contents for the The Stellar Trial summary:





Relevant literature
- Meta-Analyses
- Does 6-Minute Walk Test (6MWT) Predict Clinical Events in Pulmonary Hypertension? (1)
- The authors conducted a meta-analysis of 22 studies and searched several databases for RCTs assessing functional capacity by 6MWT, a common endpoint in PAH studies, at baseline and at the end of the follow-up period to assess the influence of PAH treatments on outcomes. They performed a meta-regression analysis to test the relationship between 6MWT and outcomes and found that improvement in 6MWT induced by treatment does not reflect a reduction in clinical outcomes.
- However, the 6MWT continues to be utilized as an endpoint in most PAH studies.
- Does 6-Minute Walk Test (6MWT) Predict Clinical Events in Pulmonary Hypertension? (1)

Relevant guidelines
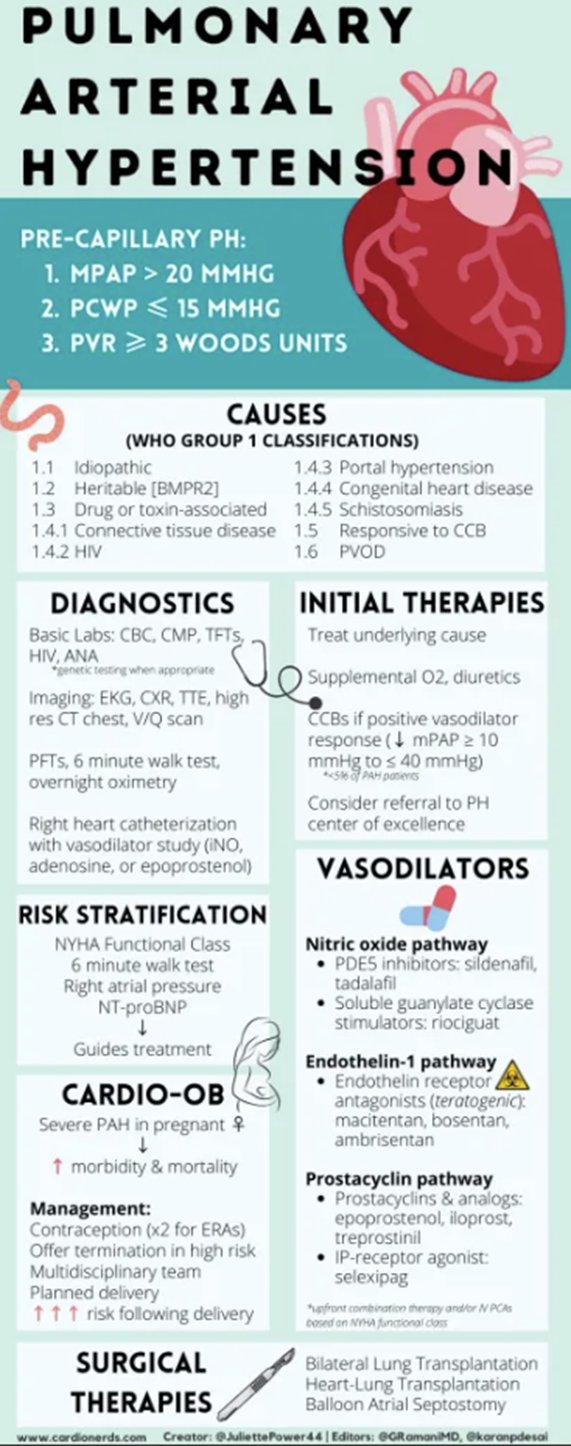
- There are three drugs approved by the US Food and Drug Administration for the treatment of group 1 PH.
- Nitric oxide (NO) pathway mediators: phosphodiesterase 5 (PDE5) inhibitors: tadalafil and sildenafil; soluble guanylate cyclase stimulator: riociguat.
- Endothelin receptor antagonists: bosentan, ambrisentan, and macitentan.
- Prostacyclin pathway agonists: prostacyclins: treprostinil (oral, inhaled, subcutaneous, or intravenous), iloprost (inhaled), and epoprostenol (intravenous or inhaled); oral prostaglandin I2 receptor agonist: selexipag.

Figure 1 ESC/ERS 2022 PAH Guidelines
Study Rationale
PAH involves proliferative remodeling of the pulmonary vessels and is a progressive disease with high mortality and morbidity. There has been minimal progress in therapies for this disease in the last decade, and it is important to continue to explore novel drug targets. Thus, this study aims to explore the efficacy of a new drug, Sotatercept, a fusion protein that traps activins and growth differentiation factors involved in pulmonary arterial hypertension.
Study Objectives
The study is a phase 3 drug trial designed to assess the efficacy, safety, and adverse-event profile of sotatercept in combination with stable background therapy in adult patients with symptomatic pulmonary arterial hypertension. Specifically, it assessed change in the 6-minute walk distance from baseline to week 24 and 9 secondary endpoints as detailed in the results.

- Trial
- Phase 3, multicenter, double-blind, randomized, placebo-controlled trial
- Intervention
- Patients stratified according to baseline WHO functional class (II vs. III) and background therapy for PAH (monotherapy or double therapy vs. triple therapy) and were randomly assigned to placebo or sotatercept
- Sotatercept or placebo was administered by subcutaneous injection every 21 days. Sotatercept was administered at a starting dose of 0.3 mg/kg at visit 1 and was escalated to the target dose of 0.7 mg/kg at visit 2 (day 21). Patients continued to receive a dose of 0.7 mg per kilogram for the duration of the trial
Enrollment Criteria

Primary Outcome
- Change from baseline at week 24 in the 6-minute walk distance.
Secondary Endpoints:
- Multicomponent improvement- measured by the percentage of patients meeting all three criteria below at week 24 relative to baseline
- Improvement in 6-minute walk distance [increase of ≥30 m]
- Improvement in NT-proBNP level [decrease of ≥30%] or maintenance or achievement of an NT-proBNP level of <300 pg per mL
- Improvement in WHO functional class [class III to II or I, or II to I] or maintenance of class II
- Change in pulmonary vascular resistance
- Change in N-terminal pro–B-type natriuretic peptide level
- Improvement in WHO functional class
- Time to the first occurrence of death or nonfatal clinical worsening event defined by death from any cause or specified nonfatal clinical worsening events
- worsening-related listing for lung or heart-lung transplantation,
- initiation or rescue therapy with an approved background treatment or increase in the prostacyclin dose by ≥10%
- atrial septostomy
- hospitalization ≥24 hours for worsening of pulmonary arterial hypertension
- worsening of pulmonary arterial hypertension relative to baseline as defined by both a worsened WHO functional class and a decrease in 6-minute walk distance by ≥15%
- French risk score- defined by the meeting of all three criteria below for low risk:
- WHO functional class I or II
- 6-minute walk distance of >440 m
- NT-proBNP level of <300 pg per milliliter
- Change from baseline in the Physical Impacts domain score of the Pulmonary Arterial Hypertension–Symptoms and Impact (PAH-SYMPACT) questionnaire
- Change from baseline in the Cardiopulmonary Symptoms Impacts domain score of the Pulmonary Arterial Hypertension–Symptoms and Impact (PAH-SYMPACT) questionnaire
- Change from baseline in the Cognitive/Emotional Impacts domain score of the Pulmonary Arterial Hypertension–Symptoms and Impact (PAH-SYMPACT) questionnaire
- **all were assessed at week 24 except time to death or clinical worsening, which was assessed when the last patient completed the week 24 visit.
Statistical Analysis
Intention-to-treat analysis. Differences between the sotatercept and placebo groups for the primary outcome were assessed for statistical significance at p<0.05.

Baseline Characteristics

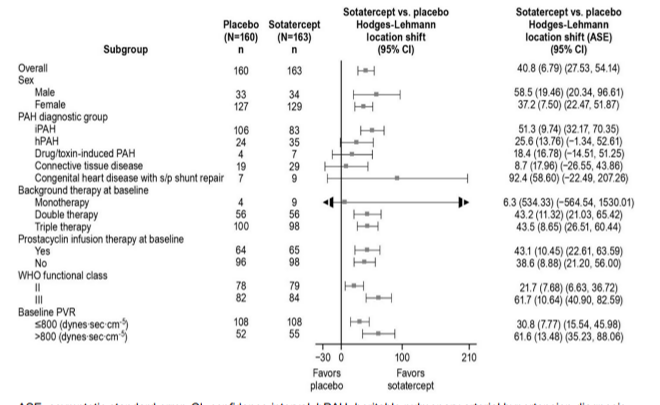
- Of the 434 participants who were eligible 323 underwent randomization (91 sites across 21 countries) to Sotatercept (n = 163) or placebo (n = 160) in combination with stable background therapy.
- 61% of randomized patients were receiving triple therapy.
- 39.9% of patients were receiving prostacyclin infusion therapy.
- Baseline demographics and clinical characteristics were similar across both groups. The mean age was 47.9 years, and the mean length of time since diagnosis was 8.8 years. 79.3% were female.
- Adherence to the trial regimen was similar across groups, 98.4% in the sotatercept group and 99% in the placebo group.
Outcomes
Primary Outcome
- There were significant improvements observed with sotatercept treatment relative to placebo for change from baseline at 24 weeks in:
- Pulmonary vascular resistance
- NT-proBNP levels
- WHO functional class
- PAH SYMPACT Questionnaire
- There was an early (week 10) significant difference in the distribution of time to first occurrence of death or nonfatal clinical worsening event in the sotatercept group and placebo group (p<0.001). At a median follow-up of 32.7 weeks, the HR in sotatercept group as compared to placebo was 0.16 (95% CI, 0.08 to 0.35).

The participants receiving the sotatercept had more significant improvements in the Physical Impacts and Cardiopulmonary Symptom domain scores in the PAH-SYMPACT quality of life questionnaire between baseline to week 24 as compared to the placebo group. There was no significant difference between the two groups for the PAH-SYMPACT Cognitive/Emotional Impacts domain score (p = 0.16)
Adverse Events
- Adverse events that occurred more frequently in the sotatercept group:
- nonserious epistaxis, gingival bleeding, telangiectasia, dizziness, thrombocytopenia, increase in hemoglobin

- Serious adverse events occurred in 23 patients (14.1%) in the sotatercept group and in 36 patients (22.5%) in the placebo group.
- One patient had a serious adverse event that led to discontinuation of sotatercept and withdrawal from the trial.



Conclusions
- The STELLAR trial demonstrated that the addition of 24 weeks of treatment of sotatercept to background therapy for pulmonary hypertension improved exercise capacity, as assessed by the 6-minute walk distance, and improved pulmonary vascular resistance, NT-proBNP levels, risk of death, and the Physical Impacts and Cardiopulmonary Symptoms domain scores of the PAH-SYMPACT quality of life questionnaire.
Limitations and Considerations:
- The STELLAR trial only enrolled WHO functional class II or III patients with certain forms of pulmonary hypertension, which may limit the generalizability of these results to higher-risk or sicker patients.
- Patients with pulmonary hypertension related to connective tissue disease, congenital heart disease, or drugs and toxins were underrepresented.
- Only patients with pulmonary hypertension with a baseline pulmonary vascular resistance of at least 400 or >5 Woods units were eligible.
- There was potential for unblinding due to side effects known to be associated with sotatercept
- It is difficult to ascertain long-term durability and safety profile given that the median treatment period in this study was 7.5 months. The ongoing SOTERIA trial is designed to explore long-term durability.
- STELLAR was not designed to study the effects of sotatercept on mortality

- Savarese G, Paolillo S, Costanzo P, et al. Does 6-minute walk test predict clinical events in pulmonary arterial hypertension? A meta-analysis of 22 studies. J Am Coll Cardiol. 2012 Mar, 59 (13_Supplement) E1601.
- Zhang H, Wei Y, Zhang C, et al. Pulmonary Artery Denervation for Pulmonary Arterial Hypertension. J Am Coll Cardiol Intv. 2022 Dec, 15 (23) 2412–2423.
- Chin K, Sitbon O, Doelberg M, et al. Three- Versus Two-Drug Therapy for Patients With Newly Diagnosed Pulmonary Arterial Hypertension. J Am Coll Cardiol. 2021 Oct, 78 (14) 1393–1403.
- Said K. Macitentan in pulmonary arterial hypertension: The SERAPHIN trial. Glob Cardiol Sci Pract. 2014 Jun 18;2014(2):26-30.
- Humbert M, McLaughlin V, Gibbs JSR, Gomberg-Maitland M, Hoeper MM, Preston IR, Souza R, Waxman A, Escribano Subias P, Feldman J, Meyer G, Montani D, Olsson KM, Manimaran S, Barnes J, Linde PG, de Oliveira Pena J, Badesch DB; PULSAR Trial Investigators. Sotatercept for the Treatment of Pulmonary Arterial Hypertension. N Engl J Med. 2021 Apr 1;384(13):1204-1215.
- Hoeper MM, Badesch DB, Ghofrani HA, Gibbs JSR, Gomberg-Maitland M, McLaughlin VV, Preston IR, Souza R, Waxman AB, Grünig E, Kopeć G, Meyer G, Olsson KM, Rosenkranz S, Xu Y, Miller B, Fowler M, Butler J, Koglin J, de Oliveira Pena J, Humbert M; STELLAR Trial Investigators. Phase 3 Trial of Sotatercept for Treatment of Pulmonary Arterial Hypertension. N Engl J Med. 2023 Apr 20;388(16):1478-1490.

Summary by: Dr. Shivani Hanchate @HanchateShivani and Dr. Maani Kamal @Kamal_mz
Visual abstract by: Dr. Yetunde Kemi Fatade @joyfuldockemi
Trial Tweets by: Dr. Ronaldo Filho @Ronaldo_CFF
Moderator of Twitter during CardsJC by: Dr. Paul Montana @PaulMontanaMD
Promo by: Student Doctor Shivani Reddy @ShivaniReddy_1
Under the guidance of House Chief: Dr. Gurleen Kaur @GurleenKaur_96 & Director of CardsJC Dr. Devesh Rai, @DeveshRaiMD
Supported by House Faculty: Dr. Ahmed Ghoneem @a_h_ghoneem, Dr. Colin Blumenthal @CBlumenthal2, and Dr. Sukriti Banthiya @sukritibanthiya
Faculty experts: Dr. Ryan Tedford @RyanTedfordMD, Dr. Mardi Gomberg-Maitland @mardigomberg, Dr. Michael Felker @DukeHFDoc, Dr. Shelley Zieroth @Shelley Zieroth, and Dr. Anjali Vaidya @anjalivaidyaMD

STELLAR Archive
- Pulmonary arterial hypertension (PAH) is hypothesized to be due to unbalanced proliferation > apoptosis in the pulmonary vasculature → remodeling & hypertension!
Dr. Gurleen Kaur (@ Gurleen_Kaur96): Pro-proliferative signaling pathways involving growth factors, cytokines, & metabolic signaling involved in pathophysiology of PAH. Therapies targeting this complex mechanism are used in PAH. Great review on mechanisms of the disease below.

Image link: https://www.nature.com/articles/nrcardio.2011.87
- An awesome infographic by @JuliettePower44PAH on PAH therapies below.
Check out these other helpful resources → The CardioNerds pulmonary hypertension archive (https://www.cardionerds.com/pulmonary-hypertension) & a summary of the approach to PH management (https://www.ahajournals.org/doi/full/10.1161/JAHA.122.029024)
- Sotatercept is a first-in-class drug distinguishes itself from existing treatments for PAH.
- It’s a fusion protein of activin receptor type IIa that traps TGF-B superfamily members re-balancing PA homeostasis.

Image link: https://www.nejm.org/doi/full/10.1056/NEJMoa2024277
Q1. In the STELLAR trial, it’s worth noting that the patient demographics revealed 80% females and 90% individuals of the white racial group. Do you believe the composition of the trial participants accurately represents the patient population typically seen in PAH clinics?
Dr. Ryan J Tedford (@RyanTedfordMD): The baseline characteristics are quite similar to other large PH studies, including ambition. However, the race imbalance may not be representative of some PH clinics.
Dr. Anjali Vaidya (@anjalivaidyaMD): Generally, yes. However, there is more heritable (18%) PAH and less CTD (only 15%) PAH represented here than our PAH practice and many other PAH clinical trials. Also, 89% white race, which is not representative.
Dr. Mardi Gomberg (@mardigomberg): I think this is the reality of our PAH trials but in DC we have a more diverse group. Women always predominate.
Dr. Robert J Bernardo (@rjbernardoMD): Minorities are still very underrepresented in PAH trials.
Dr. Ryan J Tedford (@RyanTedfordMD): I completely agree. We need to do better here.
Dr. Mardi Gomberg (@mardigomberg): I think this is often due to sites selected but there are bigger issues at play. Do you think that is based on the sites chosen, cultural issues, lack of language translation?
Q2. At baseline, 48.6% of the population were WHO FC II and 61.3% were on triple therapy. Unclear how many pts were WHO FC II on triple therapy. Would that be representative from your practice?
Dr. Ryan J Tedford (@RyanTedfordMD): Almost all are now on dual or triple therapy. I think this study cohort is representative.
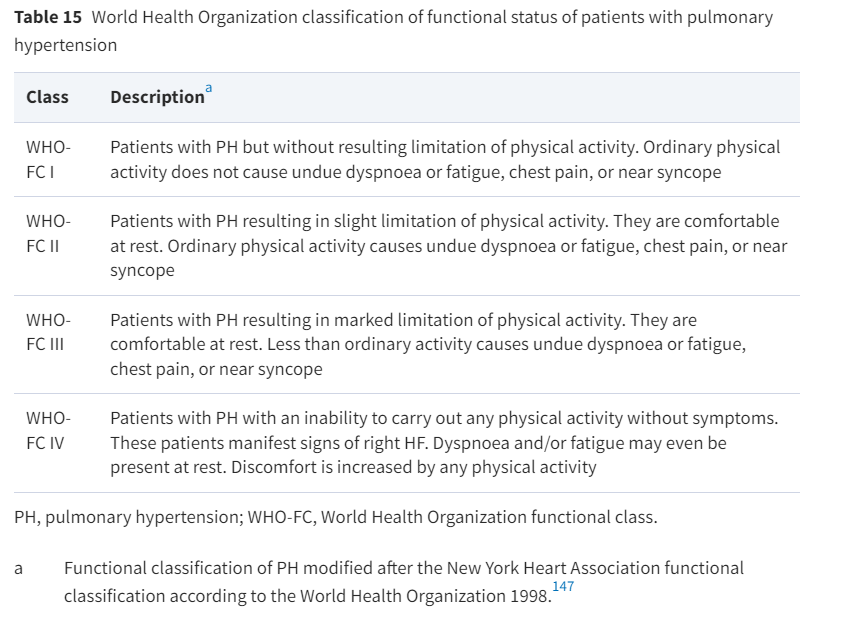
Dr. Gurleen Kaur (@ Gurleen_Kaur96): Review of WHO classification of functional status from the ESC PH guidelines below
Q3. Based on the inclusion/exclusion criteria and the high proportion of triple therapy, and low PAH hospitalization rate within 6mo from baseline, should we be more aggressive in treating PAH?
Dr. Ryan J Tedford (@RyanTedfordMD): I’m not the expert here (@mardigomberg @jeanlucvachiery @rjbernardoMD), but we need to treat to achieve a low risk profile. The good news in PAH is that we have lots of options. Provocative perspective here on aggressive afterload reduction in PAH: pubmed.ncbi.nlm.nih.gov/34905704/
Dr. PH Giessen (@GiessenPh): Agree, but should not miss to improve contractility as well…this is still a missing link.
Dr. Ryan J Tedford (@ RyanTedfordMD): Or maybe enhance lusitropy as well?
Dr. Mardi Gomberg (@mardigomberg): AMBITION proved upfront ‘aggressive’ is better than monotherapy – do we need a trial with sotatercept?
I think yes we need to be aggressive- we have always wanted to achieve low risk but didn’t have as many options. Sometimes we do reach low risk with dual, prostacyclins, and sometimes we dont what is important is following them.
I also think that we had subjects on double and triple therapy and not clearly at goal..
Dr. Robert J Bernardo (@rjbernardoMD): Agree. Most of us aim for RV reverse remodeling. #STELLAR is an important step towards that goal. The data that’ll be presented at #ERS2023 shows some of that.
Dr. Mardi Gomberg (@mardigomberg): Agree with @rjbernardoMD its all about the RV. #ERS2023 will also have some updated SOTERIA longer term exposure on sotatercept study; combined all sotatercept phase 2.
Q4. To the Results! Do you think the different combinations of background medications affected the results of this trial? If so, how?
Dr. Ryan J Tedford (@RyanTedfordMD): Probably not. Results consistent among dual and triple therapy patients. And pretty standard combinations. (Always review the supplemental data!)
Dr. Mardi Gomberg (@mardigomberg): If you still have vascular disease and not at goal it doesn’t matter what you are on @anjalivaidyaMD thoughts?
What is interesting is that subjects on parenteral therapy with one or even 2 meds improved.
Dr. Anjali Vaidya (@anjalivaidyaMD): I think that is valid @mardigomberg ! Yes, #CardsJC. If you’re not at goal, based on various Risk Assessment tools, regardless of therapy, we need to consider more therapeutic options. Target additional pathways. #ThePeoplesVentricle
Q5. Secondary endpoint (ranked hierarchical multicomponent):
1) % of pts from baseline to 24wks (all 3):
-6MWT ↑ >30m, and
-NT-proBNP ↓ ≥ 30% or < 300pg/ml, and
-Improvement or same WHO FC
Are they good clinical surrogates for clinical significant improvement?

Dr. Ryan J Tedford (@RyanTedfordMD): Again, I’m going with yes! Several studies, led by
Dr. Mardi Gomberg (@mardigomberg): In combination these are reflective of the subjects’ clinical state- in phase 2 we also saw this with PVR.
Q6. Adverse events more common w/ Sotatercept:
– ↓ Platelets
– Mild bleeding (epistaxis, gingival)
– ↑ Telangiectasia
– Headache
– Diarrhea
– Dizziness
Do you think Sotatercept adverse events were clinically relevant?

Dr. Ryan J Tedford (@RyanTedfordMD): We need to point out that many fewer AEs with study drug than placebo! Increase in Hgb is interesting especially as we study other populations. We will need to get an eye on telangiectasias – though thankfully no significant bleeding in this study.
Dr. Anjali Vaidya (@anjalivaidyaMD): Agree @RyanTedfordMD, the lack of significant bleeding is reassuring. Though we all await and look forward to more real-world clinical experience and observation.
Dr. Mardi Gomberg (@mardigomberg): We expected an increase in hemoglobin and managed this during the study without issue, the telangiectasia were seen and may indicate better responders, no GIB from them.
Dr. Anjali Vaidya (@anjalivaidyaMD): I agree with @mardigomberg – credit for being a major site on the trial and her experience – but yes, while the side effects are relatively ‘novel’ in our space, with more experience and observation, our comfort will grow. There doesn’t seem to be signal for dangerous AEs.
Dr. Sudarshan Rajagopal (@SudarRajagopal): I’d like to see long-term safety data before using in lower risk patients – when do the bleeds happen? The OLE will be helpful to know if it is an upfront risk or something that compounds with time.
Dr. Mardi Gomberg (@mardigomberg): Additional comment on AEs- some had symptoms of an ‘increase in prostacyclin’ they didn’t need as much – this is a hot topic!
Q7. Sotatercept improved 6MWD (primary endpoint). Its safety profile is favorable. STELLAR trial was not designed/powered to evaluate mortality. Would you expect it to reduce mortality in future trials?
Dr. Anjali Vaidya (@anjalivaidyaMD): Important to note, credit to #STELLAR, that avg duration of PAH diagnosis prior to enrollment was 9 years! with 61% on triple therapy and 39% on PGI2 based therapy. Thus, hitting the primary and nearly all secondary endpoints in a short time was quite impressive.
Dr. Mardi Gomberg (@mardigomberg): Mortality will be hard to show in clinical trials especially as we are closer to normalizing pressure-maybe in Zenith the int-high/high risk subjects may show a trend.
Mortality benefit need larger numbers as well but cure=cure, our real goal!
Dr. Ryan J Tedford (@RyanTedfordMD): Agree w/ @mardigomberg and @anjalivaidyaMD. We may also gain some insight from the open label long term follow up study #Soteria for those who have completed randomized studies.
Q8. Are the benefits of sotatercept in PAH observed in this trial believable?
Dr. Ryan J Tedford (@RyanTedfordMD): The results are quite ‘Stellar’ – but consistent with PULSAR Phase 2 data. Keep in mind that 60% of patients did NOT meet the multicomponent-improvement measure. So very good but still lots of room to improve.
Dr. Mardi Gomberg (@mardigomberg): As the first target that is not a primary vasodilatory YES!
Q9. Do you think STELLAR trial will change our practice? Will you consider prescribing sotatercept to your patients? Why / Why not?
Dr. Mardi Gomberg (@mardigomberg): Once approved and available for home use absolutely. Can we continue to develop new therapies- a definitive YES! Looking forward to results of Zenith and Hyperion as well, and off topic for today CANENCE- PH-LHD sotatercept study.
Dr. Ryan J Tedford (@RyanTedfordMD): YES, once approved!
Q10. Sotatercept is SC every 3 wks which is relatively convenient, should it be evaluated as an initial drug in PAH?
Dr. Sudarshan Rajagopal (@SudarRajagopal): Way more convenient than prostacyclins which require uptitration with side effects of headache, nausea, vomiting and diarrhea. It will probably not take the place of PDE5i + ERA but may be used before prostacyclin.
Dr. Anjali Vaidya (@anjalivaidyaMD): The question of ‘when’ to implement Sotatercept remains a big one! we in the field have been discussing and anticipating and wondering for at least a year. It is not to be ‘monotherapy’ given the standards of care established in the PAH field….
Dr. Ryan J Tedford (@RyanTedfordMD): Yes agree – probably hard to do a ethical study, just like in HFrEF – we have added to SOC therapies.
Dr. Kurt Prins (@kurt_prins): My personal approach will be to give to nearly everyone as long as it’s affordable. Hemodynamic data are impressive! Time will tell how to be implement it though!
Dr. Robert J Bernardo (@rjbernardoMD): Million dollar question. Do we use it upfront with dual oral therapy? Do we use it at the time we start PGI2? Do we do it as rescue therapy?
Probably the earlier the better, to enhance RV reverse remodeling.
Dr. Sandeep Sahay (@SandeepSahayMD): Trial is on going at present in newly diagnosed patients with pah. https://classic.clinicaltrials.gov/ct2/show/NCT04811092…
Dr. Steven C. Stroud (@ChaseStroudMD): Many logistical issues to be answered… administering site, role of specialty pharmacy, and what will be the pathway for our medicaid / under-insured patients? Exciting times all the same!
Q11. Sotatercept long-term efficacy and profile safety is unknown. The open-label ongoing SOTERIA trial aims to help sorting this out. Any final thoughts about the trial?
Dr. Sudarshan Rajagopal (@SudarRajagopal): Hopefully will have translational studies that identify molecular signatures of super-responders and whether it is more efficacious in patients with BMPR2 mutations. But hugely important trial – most excited the field has been since AMBITION.
Finally, don’t miss another amazing #CNstatsdemystified by @RonaldoCCF on Hodges-Lehmann (HL) estimator https://twitter.com/Ronaldo_CFF/status/1696616425756950641



